Manual of Surgery, Alexis Thomson [new books to read txt] 📗
- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery, Alexis Thomson [new books to read txt] 📗». Author Alexis Thomson
Moist Gangrene is an acute process, the dead part retaining its fluids and so affording a favourable soil for the development of bacteria. The action of the organisms and their toxins on the adjacent tissues leads to a rapid and wide spread of the process. The skin becomes moist and macerated, and bullæ, containing dark-coloured fluid or gases, form under the epidermis. The putrefactive gases evolved cause the skin to become emphysematous and crepitant and produce an offensive odour. The tissues assume a greenish-black colour from the formation in them of a sulphide of iron resulting from decomposition of the blood pigment. Under certain conditions the dead part may undergo changes resembling more closely those of ordinary post-mortem decomposition. Owing to its nature the spread of the gangrene is seldom arrested by the natural protective processes, and it usually continues until the condition proves fatal from the absorption of toxins into the circulation.
The clinical features vary in the different varieties of moist gangrene, but the local results of bacterial action and the constitutional disturbance associated with toxin absorption are present in all; the prognosis therefore is grave in the extreme.
From what has been said, it will be gathered that in dry gangrene there is no urgent call for operation to save the patient's life, the primary indication being to prevent the access of bacteria to the dead part, and especially to the surface exposed at the line of demarcation. In moist gangrene, on the contrary, organisms having already obtained a footing, immediate removal of the dead and dying tissues, as a rule, offers the only hope of saving life.
Varieties of Gangrene Varieties of Gangrene essentially due to Interference with the CirculationWhile the varieties of gangrene included in this group depend primarily on interference with the circulation, it is to be borne in mind that the clinical course of the affection may be profoundly influenced by superadded infection with micro-organisms. Although the bacteria do not play the most important part in producing tissue necrosis, their subsequent introduction is an accident of such importance that it may change the whole aspect of affairs and convert a dry form of gangrene into one of the moist type. Moreover, the low state of vitality of the tissues, and the extreme difficulty of securing and maintaining asepsis, make it a sequel of great frequency.
Senile Gangrene.—Senile gangrene is the commonest example of local death produced by a gradual diminution in the quantity of blood passing through the parts, as a result of arterio-sclerosis or other chronic disease of the arteries leading to diminution of their calibre. It is the most characteristic example of the dry type of gangrene. As the term indicates, it occurs in old persons, but the patient's age is to be reckoned by the condition of his arteries rather than by the number of his years. Thus the vessels of a comparatively young man who has suffered from syphilis and been addicted to alcohol are more liable to atheromatous degeneration leading to this form of gangrene than are those of a much older man who has lived a regular and abstemious life. This form of gangrene is much more common in men than in women. While it usually attacks only one foot, it is not uncommon for the other foot to be affected after an interval, and in some cases it is bilateral from the outset. It must clearly be understood that any form of gangrene may occur in old persons, the term senile being here restricted to that variety which results from arterio-sclerosis.
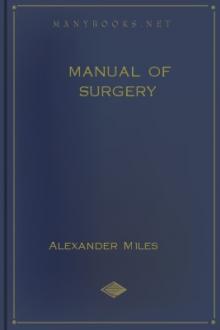
Fig. 20.—Senile Gangrene of the Foot, showing line of demarcation.
Clinical Features.—The commonest seat of the disease is in the toes, especially the great toe, whence it spreads up the foot to the heel, or even to the leg (Fig. 20). There is often a history of some slight injury preceding its onset. The vitality of the tissues is so low that the balance between life and death may be turned by the most trivial injury, such as a cut while paring a toe-nail or a corn, a blister caused by an ill-fitting shoe or the contact of a hot-bottle. In some cases the actual gangrene is determined by thrombosis of the popliteal or tibial arteries, which are already narrowed by obliterating endarteritis.
It is common to find that the patient has been troubled for a long time before the onset of definite signs of gangrene, with cold feet, with tingling and loss of feeling, or a peculiar sensation as if walking on cotton wool.
The first evidence of the death of the part varies in different cases. Sometimes a dark-blue spot appears on the medial side of the great toe and gradually increases in size; or a blister containing blood-stained fluid may form. Streaks or patches of dark-blue mottling appear higher up on the foot or leg. In other cases a small sore surrounded by a congested areola forms in relation to the nail and refuses to heal. Such sores on the toes of old persons are always to be looked upon with suspicion and treated with the greatest care; and the urine should be examined for sugar. There is often severe, deep-seated pain of a neuralgic character, with cramps in the limb, and these may persist long after a line of demarcation has formed. The dying part loses sensibility to touch and becomes cold and shrivelled.
All the physical appearances and clinical symptoms associated with dry gangrene supervene, and the dead portion is delimited by a line of demarcation. If this forms slowly and irregularly it indicates a very unsatisfactory condition of the circulation; while, if it forms quickly and decidedly, the presumption is that the circulation in the parts above is fairly good. The separation of the dead part is always attended with the risk of infection taking place, and should this occur, the temperature rises and other evidences of toxæmia appear.
Prophylaxis.—The toes and feet of old people, the condition of whose circulation predisposes them to gangrene, should be protected from slight injuries such as may be received while paring nails, cutting corns, or wearing ill-fitting boots. The patient should also be warned of the risk of exposure to cold, the use of hot-bottles, and of placing the feet near a fire. Attempts have been made to improve the peripheral circulation by establishing an anastomosis between the main artery of a limb and its companion vein, so that arterial blood may reach the peripheral capillaries—reversal of the circulation—but the clinical results have proved disappointing. (See Op. Surg., p. 29.)
Treatment.—When there is evidence that gangrene has occurred, the first indication is to prevent infection by purifying the part, and after careful drying to wrap it in a thick layer of absorbent and antiseptic wool, retained in place by a loosely applied bandage. A slight degree of elevation of the limb is an advantage, but it must not be sufficient to diminish the amount of blood entering the part. Hot-bottles are to be used with the utmost caution. As absolute dryness is essential, ointments or other greasy dressings are to be avoided, as they tend to prevent evaporation from the skin. Opium should be given freely to alleviate pain. Stimulation is to be avoided, and the patient should be carefully dieted.
When the gangrene is limited to the toes in old and feeble patients, some surgeons advocate the expectant method of treatment, waiting for a line of demarcation to form and allowing the dead part to be separated. This takes place so slowly, however, that it necessitates the patient being laid up for many weeks, or even months; and we agree with the majority in advising early amputation.
In this connection it is worthy of note that there are certain points at which gangrene naturally tends to become arrested—namely, at the highly vascular areas in the neighbourhood of joints. Thus gangrene of the great toe often stops when it reaches the metatarso-phalangeal joint; or if it trespasses this limit it may be arrested either at the tarso-metatarsal or at the ankle joint. If these be passed, it usually spreads up the leg to just below the knee before signs of arrestment appear. Further, it is seen from pathological specimens that the spread is greater on the dorsal than on the plantar aspect, and that the death of skin and subcutaneous tissues extends higher than that of bone and muscle.
These facts furnish us with indications as to the seat and method of amputation. Experience has proved that in senile gangrene of the lower extremity the most reliable and satisfactory results are obtained by amputating in the region of the knee, care being taken to perform the operation so as to leave the prepatellar anastomosis intact by retaining the patella in the anterior flap. The most satisfactory operation in these cases is Gritti's supra-condylar amputation. Hæmorrhage is easily controlled by digital pressure, and the use of a tourniquet should be dispensed with, as the constriction of the limb is liable to interfere with the vitality of the flaps.
When the tibial vessels can be felt pulsating at the ankle it may be justifiable, if the patient urgently desires it, to amputate lower than the knee; but there is considerable risk of gangrene recurring in the stump and necessitating a second operation.
That amputation for senile gangrene performed between the ankle and the knee seldom succeeds, is explained by the fact that the vascular obstruction is usually in the upper part of the posterior tibial artery, and the operation is therefore performed through tissues with an inadequate blood supply. It is not uncommon, indeed, on amputating above the knee, to find even the popliteal artery plugged by a clot. This should be removed at the amputation by squeezing the vessel from above downward by a “milking” movement, or by “catheterising the artery” with the aid of a cannula with a terminal aperture.
It is to be borne in mind that the object of amputation in these cases is merely to remove the gangrenous part, and so relieve the patient of the discomfort and the risks from infection which its presence involves. While it is true that in many of these patients the operation is borne remarkably well, it must be borne in mind that those who suffer from senile gangrene are of necessity bad lives, and a guarded opinion should be expressed as to the prospects of survival. The possibility of the disease developing in the other limb has already been referred to.
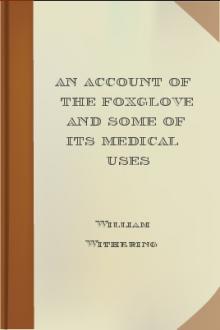
Fig. 21.—Embolic Gangrene of Hand and Arm.
Embolic Gangrene (Fig. 21).—This is the most typical form of gangrene resulting from the sudden occlusion of the main artery of a part, whether by the impaction of an embolus or the formation of a thrombus in its lumen, when the collateral circulation is not sufficiently free to maintain the vitality of the tissues.
There is sudden pain at the site of impaction of the embolus, and the pulses beyond are lost. The limb becomes cold, numb, insensitive, and powerless. It is often pale at first—hence the term “white gangrene” sometimes applicable to the early appearances, which closely




Comments (0)