Manual of Surgery, Alexis Thomson [new books to read txt] 📗
- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery, Alexis Thomson [new books to read txt] 📗». Author Alexis Thomson
Electrolysis acts by decomposing the blood and tissues into their constituent elements—oxygen and acids appearing at the positive, hydrogen and bases at the negative electrode. These substances and gases being given off in a nascent condition, at once enter into new combinations with anything in the vicinity with which they have a chemical affinity. In the nævus the practical result of this reaction is that at the positive pole nitric acid, and at the negative pole caustic potash, both in a state of minute subdivision, make their appearance. The effect on the tissues around the positive pole, therefore, is equivalent to that of an acid cauterisation, and on those round the negative pole, to an alkaline cauterisation.
As the process is painful, a general anæsthetic is necessary. The current used should be from 20 to 80 milliampères, gradually increasing from zero, without shock; three to six large Bunsen cells give a sufficient current, and no galvanometer is required. Steel needles, insulated with vulcanite to within an eighth of an inch of their points, are the best. Both poles are introduced into the nævus, the positive being kept fixed at one spot, while the negative is moved about so as to produce a number of different tracks of cauterisation. On no account must either pole be allowed to come in contact with the skin, lest a slough be formed. The duration of the sitting is determined by the effect produced, as indicated by the hardening of the tumour, the average duration being from fifteen to twenty minutes. If pallor of the skin appears, it indicates that the needles are too near the surface, or that the blood supply to the integument is being cut off, and is an indication to stop. To cauterise the track and so prevent bleeding, the needles should be slowly withdrawn while the current is flowing. When the skin is reached the current is turned off. The punctures are covered with collodion. Six or eight weeks should be allowed to elapse before repeating the procedure. From two to eight or ten sittings may be necessary, according to the size and character of the nævus.
Excision is to be preferred for nævi of moderate size situated on covered parts of the body, where a scar is of no importance. Its chief advantages over electrolysis are that a single operation is sufficient, and that the cure is speedy and certain. The operation is attended with much less hæmorrhage than might be expected.
Cavernous Angioma.—This form of angioma consists of a series of large blood spaces which are usually derived from the dilatation of the capillaries of a subcutaneous nævus. The spaces come to communicate freely with one another by the disappearance of adjacent capillary walls. While the most common situation is in the subcutaneous tissue, a cavernous angioma is sometimes met with in internal organs. It may appear at any age from early youth to middle life, and is of slow growth and may become stationary. The swelling is rounded or oval, there is no pulsation or bruit, and the tumour is but slightly compressible. The treatment consists in dissecting it out.
Aneurysm by Anastomosis is the name applied to a vascular tumour in which the arteries, veins, and capillaries are all involved. It is met with chiefly on the upper part of the trunk, the neck, and the scalp. It tends gradually to increase in size, and may, after many years, attain an enormous size. The tumour is ill-defined, and varies in consistence. It is pulsatile, and a systolic bruit or a “thrilling” murmur may be heard over it. The chief risk is hæmorrhage from injury or ulceration.
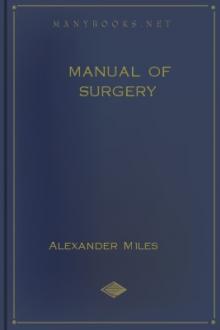
Fig. 69.—Cirsoid Aneurysm of Forehead in a boy æt. 10.
(Mr. J. W. Dowden's case.)
The treatment is conducted on the same lines as for nævus. When electrolysis is employed, it should be directed towards the afferent vessels; and if it fails to arrest the flow through these, it is useless to persist with it. In some cases ligation of the afferent vessels has been successful.
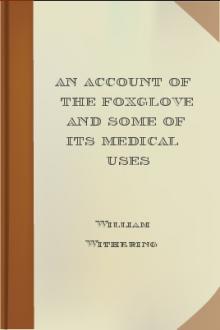
Fig. 70.—Cirsoid Aneurysm of Orbit and Face, which developed after a blow on the Orbit with a cricket ball.
(From a photograph lent by Sir Montagu Cotterill.)
Arterial Angioma or Cirsoid Aneurysm.—This is composed of the enlarged branches of an arterial trunk. It originates in the smaller branches of an artery—usually the temporal—and may spread to the main trunk, and may even involve branches of other trunks with which the affected artery anastomoses.
The condition is probably congenital in origin, though its appearance is frequently preceded by an injury. It almost invariably occurs in the scalp, and is usually met with in adolescent young adults.
The affected vessels slowly increase in size, and become tortuous, with narrowings and dilatations here and there. Grooves and gutters are frequently found in the bone underlying the dilated vessels.
There is a constant loud bruit in the tumour, which greatly troubles the patient and may interfere with sleep. There is no tendency either to natural cure or to rupture, but severe and even fatal hæmorrhage may follow a wound of the dilated vessels.
The condition may be treated by excision or by electrolysis. In excision the hæmorrhage is controlled by an elastic tourniquet applied horizontally round the head, or by ligation of the feeding trunks. In large tumours the bleeding is formidable. In many cases electrolysis is to be preferred, and is performed in the same way as for nævus. The positive pole is placed in the centre of the tumour, while the negative is introduced into the main affluents one after another.
ANEURYSMAn aneurysm is a sac communicating with an artery, and containing fluid or coagulated blood.
Two types are met with—the pathological and the traumatic. It is convenient to describe in this section also certain conditions in which there is an abnormal communication between an artery and a vein—arterio-venous aneurysm.
Pathological AneurysmIn this class are included such dilatations as result from weakening of the arterial coats, combined, in most cases, with a loss of elasticity in the walls and increase in the arterial tension due to arterio-sclerosis. In some cases the vessel wall is softened by arteritis—especially the embolic form—so that it yields before the pressure of the blood.
Repeated and sudden raising of the arterial tension, as a result, for example, of violent muscular efforts or of excessive indulgence in alcohol, plays an important part in the causation of aneurysm. These factors probably explain the comparative frequency of aneurysm in those who follow such arduous occupations as soldiers, sailors, dock-labourers, and navvies. In these classes the condition usually manifests itself between the ages of thirty and fifty—that is, when the vessels are beginning to degenerate, although the heart is still vigorous and the men are hard at work. The comparative immunity of women may also be explained by the less severe muscular strain involved by their occupations and recreations.
Syphilis plays an important part in the production of aneurysm, probably by predisposing the patient to arterio-sclerosis and atheroma, and inducing an increase in the vascular tension in the peripheral vessels, from loss of elasticity of the vessel wall and narrowing of the lumen as a result of syphilitic arteritis. It is a striking fact that aneurysm is seldom met with in women who have not suffered from syphilis.
Varieties—Fusiform Aneurysm.—When the whole circumference of an artery has been weakened, the tension of the blood causes the walls to dilate uniformly, so that a fusiform or tubular aneurysm results. All the coats of the vessel are stretched and form the sac of the aneurysm, and the affected portion is not only dilated but is also increased in length. This form is chiefly met with in the arch of the aorta, but may occur in any of the main arterial trunks. As the sac of the aneurysm includes all three coats, and as the inner and outer coats are usually thickened by the deposit in them of connective tissue, this variety increases in size slowly and seldom gives rise to urgent symptoms.
As a rule a fusiform aneurysm contains fluid blood, but when the intima is roughened by disease, especially in the form of calcareous plates, shreds of clot may adhere to it.
It has little tendency to natural cure, although this is occasionally effected by the emerging artery becoming occluded by a clot; it has also little tendency to rupture.
Sacculated Aneurysm.—When a limited area of the vessel wall is weakened—for example by atheroma or by other form of arteritis—this portion yields before the pressure of the blood, and a sacculated aneurysm results. The internal and middle coats being already damaged, or, it may be, destroyed, by the primary disease, the stress falls on the external coat, which in the majority of cases constitutes the sac. To withstand the pressure the external coat becomes thickened, and as the aneurysm increases in size it forms adhesions to surrounding tissues, so that fasciæ, tendons, nerves, and other structures may be found matted together in its wall. The wall is further strengthened by the deposit on its inner aspect of blood-clot, which may eventually become organised.
The contents of the sac consist of fluid blood and a varying amount of clot which is deposited in concentric layers on the inner aspect of the sac, where it forms a pale, striated, firm mass, which constitutes a laminated clot. Near the blood-current the clot is soft, red, and friable (Fig. 72). The laminated clot not only strengthens the sac, enabling it to resist the blood-pressure and so prevent rupture, but, if it increases sufficiently to fill the cavity, may bring about cure. The principle upon which all methods of treatment are based is to imitate nature in producing such a clot.
Sacculated aneurysm, as compared with the fusiform variety, tends to rupture and also to cure by the formation of laminated clot; natural cure is sometimes all but complete when extension and rupture occur and cause death.
An aneurysm is said to be diffused when the sac ruptures and the blood escapes into the cellular tissue.
Clinical Features of Aneurysm.—Surgically, the sacculated is by far the most important variety. The outstanding feature is the existence in the line of an artery of a globular swelling, which pulsates. The pulsation is of an expansile character, which is detected by observing that when both hands are placed over the swelling they are separated with each beat of the heart. If the main artery be compressed on the cardiac side of the swelling, the pulsation is arrested and the tumour becomes smaller and less tense, and it may be still further reduced in size by gentle pressure being made over it so as to empty it of fluid blood. On allowing the blood again to flow through the artery, the pulsation returns at once, but several beats are required before the sac regains its former size. In most cases a distinct thrill is felt on placing the hand over the swelling, and a blowing, systolic murmur may be heard with the stethoscope. It is to be borne in mind that occasionally, when the interchange of blood between an aneurysm and the artery from which it arises is small, pulsation and bruit may be slight or even absent. This is also the case when the sac contains a considerable quantity of clot. When it becomes filled with clot—consolidated aneurysm—these signs disappear, and the clinical features are those of a solid tumour lying in contact with an artery, and transmitting its pulsation.
A comparison of the pulse in the artery beyond the seat of the aneurysm with that in the corresponding artery on the healthy side, shows that on the affected side the




Comments (0)