Manual of Surgery, Alexis Thomson [new books to read txt] 📗
- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery, Alexis Thomson [new books to read txt] 📗». Author Alexis Thomson
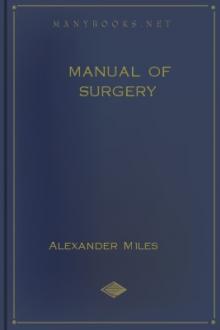
Fig. 71.—Radiogram of Aneurysm of Aorta, showing laminated clot and erosion of bodies of vertebræ. The intervertebral discs are intact.
An aneurysm exerts pressure on the surrounding structures, which are usually thickened and adherent to it and to one another. Adjacent veins may be so compressed that congestion and œdema of the parts beyond are produced. Pain, disturbances of sensation, and muscular paralyses may result from pressure on nerves. Such bones as the sternum and vertebræ undergo erosion and are absorbed by the gradually increasing pressure of the aneurysm. Cartilage, on the other hand, being elastic, yields before the pressure, so that the intervertebral discs or the costal cartilages may escape while the adjacent bones are destroyed (Fig. 71). The skin over the tumour becomes thinned and stretched, until finally a slough forms, and when it separates hæmorrhage takes place.
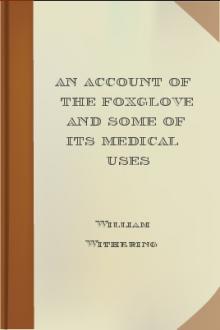
Fig. 72.—Sacculated Aneurysm of Abdominal Aorta nearly filled with laminated clot. Note greater density of clot towards periphery.
In the progress of an aneurysm towards rupture, timely clotting may avert death for the moment, but while extension in one direction has been arrested there is apt to be extension in another, with imminence of rupture, or it may be again postponed.
Differential Diagnosis.—The diagnosis is to be made from other pulsatile swellings. Pulsation is sometimes transmitted from a large artery to a tumour, a mass of enlarged lymph glands, or an inflammatory swelling which lies in its vicinity, but the pulsation is not expansile—a most important point in differential diagnosis. Such swellings may, by appropriate manipulation, be moved from the artery and the pulsation ceases, and compression of the artery on the cardiac side of the swelling, although it arrests the pulsation, does not produce any diminution in the size or tension of the swelling, and when the pressure is removed the pulsation is restored immediately.
Fluid swellings overlying an artery, such as cysts, abscesses, or enlarged bursæ, may closely simulate aneurysm. An apparent expansion may accompany the pulsation, but careful examination usually enables this to be distinguished from the true expansion of an aneurysm. Compression of the artery makes no difference in the size or tension of the swelling.
Vascular tumours, such as sarcoma and goitre, may yield an expansile pulsation and a soft, whifling bruit, but they differ from an aneurysm in that they are not diminished in size by compression of the main artery, nor can they be emptied by pressure.
The exaggerated pulsation sometimes observed in the abdominal aorta, the “pulsating aorta” seen in women, should not be mistaken for aneurysm.
Prognosis.—When natural cure occurs it is usually brought about by the formation of laminated clot, which gradually increases in amount till it fills the sac. Sometimes a portion of the clot in the sac is separated and becomes impacted as an embolus in the artery beyond, leading to thrombosis which first occludes the artery and then extends into the sac.
The progress of natural cure is indicated by the aneurysm becoming smaller, firmer, less expansile, and less compressible; the murmur and thrill diminish and the pressure effects become less marked. When the cure is complete the expansile pulsation is lost, and there remains a firm swelling attached to the vessel (consolidated aneurysm). While these changes are taking place the collateral arteries become enlarged, and an anastomotic circulation is established.
An aneurysm may prove fatal by exerting pressure on important structures, by causing syncope, by rupture, or from the occurrence of suppuration. Pressure symptoms are usually most serious from aneurysms situated in the neck, thorax, or skull. Sudden fatal syncope is not infrequent in cases of aneurysm of the thoracic aorta.
Rupture may take place through the skin, on a mucous or serous surface, or into the cellular tissue. The first hæmorrhage is often slight and stops naturally, but it soon recurs, and is so profuse, especially when the blood escapes externally, that it rapidly proves fatal. When the bleeding takes place into the cellular tissue, the aneurysm is said to become diffused, and the extravasated blood spreads widely through the tissues, exerting great pressure on the surrounding structures.
The clinical features associated with rupture are sudden and severe pain in the part, and the patient becomes pale, cold, and faint. If a comparatively small escape of blood takes place into the tissues, the sudden alteration in the size, shape, and tension of the aneurysm, together with loss of pulsation, may be the only local signs. When the bleeding is profuse, however, the parts beyond the aneurysm become greatly swollen, livid, and cold, and the pulse beyond is completely lost. The arrest of the blood supply may result in gangrene. Sometimes the pressure of the extravasated blood causes the skin to slough and, later, give way, and fatal hæmorrhage results.
The treatment is carried out on the same lines as for a ruptured artery (p. 261), it being remembered, however, that the artery is diseased and does not lend itself to reconstructive procedures.
Suppuration may occur in the vicinity of an aneurysm, and the aneurysm may burst into the abscess which forms, so that when the latter points the pus is mixed with broken-down blood-clot, and finally free hæmorrhage takes place. It has more than once happened that a surgeon has incised such an abscess without having recognised its association with aneurysm, with tragic results.
Treatment.—In treating an aneurysm, the indications are to imitate Nature's method of cure by means of laminated clot.
Constitutional treatment consists in taking measures to reduce the arterial tension and to diminish the force of the heart's action. The patient must be kept in bed. A dry and non-stimulating diet is indicated, the quantity being gradually reduced till it is just sufficient to maintain nutrition. Saline purges are employed to reduce the vascular tension. The benefit derived from potassium iodide administered in full doses, as first recommended by George W. Balfour, probably depends on its depressing action on the heart and its therapeutic benefit in syphilis. Pain or restlessness may call for the use of opiates, of which heroin is the most efficient.
Local Treatment.—When constitutional treatment fails, local measures must be adopted, and many methods are available.
Endo-aneurysmorrhaphy.—The operation devised by Rudolf Matas in 1888 aims at closing the opening between the sac and its feeding artery, and in addition, folding the wall of the sac in such a way as to leave no vacant space. If there is marked disease of the vessel, Matas' operation is not possible and recourse is then had to ligation of the artery just above the sac.
Extirpation of the Sac—The Old Operation.—The procedure which goes by this name consists in exposing the aneurysm, incising the sac, clearing out the clots, and ligating the artery above and below the sac. This method is suitable to sacculated aneurysm of the limbs, so long as they are circumscribed and free from complications. It has been successfully practised also in aneurysm of the subclavian, carotid, and external iliac arteries. It is not applicable to cases in which there is such a degree of atheroma as would interfere with the successful ligation of the artery. The continuity of the artery may be restored by grafting into the gap left after excision of the sac a segment of the great saphena vein.
Ligation of the Artery.—The object of tying the artery is to diminish or to arrest the flow of blood through the aneurysm so that the blood coagulates both in the sac and in the feeding artery. The ligature may be applied on the cardiac side of the aneurysm—proximal ligation, or to the artery beyond—distal ligation.
Proximal Ligation.—The ligature may be applied immediately above the sac (Anel, 1710) or at a distance above (John Hunter, 1785). The Hunterian operation ensures that the ligature is applied to a part of the artery that is presumably healthy and where relations are undisturbed by the proximity of the sac; the best example is the ligation of the superficial femoral artery in Scarpa's triangle or in Hunter's canal for popliteal aneurysm; it is on record that Syme performed this operation with cure of the aneurysm on thirty-nine occasions.
It is to be noted that the Hunterian ligature does not aim at arresting the flow of blood through the sac, but is designed so to diminish its volume and force as to favour the deposition within the sac of laminated clot. The development of the collateral circulation which follows upon ligation of the artery at a distance above the sac may be attended with just that amount of return stream which favours the deposit of laminated clot, and consequently the cure of the aneurysm; the return stream may, however, be so forcible as to prevent coagulation of the blood in the sac, or only to allow of the formation of a red thrombus which may in its turn be dispersed so that pulsation in the sac recurs. This does not necessarily imply failure to cure, as the recurrent pulsation may only be temporary; the formation of laminated clot may ultimately take place and lead to consolidation of the aneurysm.
The least desirable result of the Hunterian ligature is met with in cases where, owing to widespread arterial disease, the collateral circulation does not develop and gangrene of the limb supervenes.
Anel's ligature is only practised as part of the operation which deals with the sac directly.
Distal Ligation.—The tying of the artery beyond the sac, or of its two branches where it bifurcates (Brasdor, 1760, and Wardrop, 1825), may arrest or only diminish the flow of blood through the sac. It is less successful than the proximal ligature, and is therefore restricted to aneurysms so situated as not to be amenable to other methods; for example, in aneurysm of the common carotid near its origin, the artery may be ligated near its bifurcation, or in aneurysm of the innominate artery, the carotid and subclavian arteries are tied at the seat of election.
Compression.—Digital compression of the feeding artery has been given up except as a preparation for operations on the sac with a view to favouring the development of a collateral circulation.
Macewen's acupuncture or “needling” consists in passing one or more fine, highly tempered steel needles through the tissues overlying the aneurysm, and through its outer wall. The needles are made to touch the opposite wall of the sac, and the pulsation of the aneurysm imparts a movement to them which causes them to scarify the inner surface of the sac. White thrombus forms on the rough surface produced, and leads to further coagulation. The needles may be left in position for some hours, being shifted from time to time, the projecting ends being surrounded with sterile gauze.
The Moore-Corradi method consists in introducing through the wall of the aneurysm a hollow insulated needle, through the lumen of which from 10 to 20 feet of highly drawn silver or other wire is passed into the sac, where it coils up into an open meshwork (Fig. 73). The positive pole of a galvanic battery is attached to the wire, and the negative pole placed over the patient's back. A current, varying in strength from 20 to 70 milliampères, is allowed to flow for about an hour. The hollow needle is then withdrawn, but the wire is left in situ. The results are somewhat similar to those obtained by needling, but the clot formed on the large coil of wire is more extensive.




Comments (0)